

Miastenia gra vis is an autoimmune disorder characterized by abnormal and progressive weakness of skeletal muscle that is used constantly and is accompanied by fatigue during recess beraktivitas.Bila patients, so there is no muscle power will soon recover. This disease occurs due to disruption or synaptic transmission at the neuromuscular junction.
vis is an autoimmune disorder characterized by abnormal and progressive weakness of skeletal muscle that is used constantly and is accompanied by fatigue during recess beraktivitas.Bila patients, so there is no muscle power will soon recover. This disease occurs due to disruption or synaptic transmission at the neuromuscular junction.
Epidemiology
Miastenia gravis is a rare disease, and can occur at any age. This disease is usually more often seen at the age of 20-50 years. Women more often than men suffer from this disease. Ratio of women and men who suffer miastenia gravis is 6: 4. In women, this disease appears early in life, which is about 28 years, whereas in men, the disease often occurs at the age of 42 years.
ANATOMY, PHYSIOLOGICAL, and biochemical neuromuscular junction
a. Anatomy of the neuromuscular junction
Before an understanding of miastenia gravis, knowledge of anatomy and normal function of the neuromuscular junction is very important. Every normal nerve fibers branched several times and stimulated three to several hundred skeletal muscle fibers. nerve endings to create a connection called the neuromuscular junction or the neuromuscular junction. Part of motor nerve terminals eventually called the ball wide on the terminal, which lies in between the cracks found along nerve fibers. Presinaptik membrane (membrane of the nerve), post-synaptic membrane (membrane of the muscle), and the synapse is a gap to form part of the neuromuscular junction.
b. Neuromuscular Physiology and Bi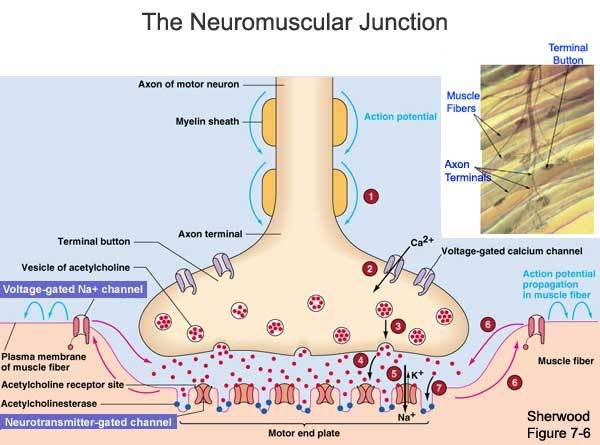 ochemistry
ochemistry
Synapse is the gap between the membrane and presinaptik post synaptic membrane. Ranged from 20-30 nanometers wide and filled by a basal lamina, which is a thin layer of reticular fibers as the foam that can be passed by the extracellular fluid by diffusion. Presinaptik terminals containing acetylcholine-containing vesicles in it (ACH). Acetylcholine is synthesized in the cytoplasm terminal, but quickly absorbed into the small number of synaptic vesicles, which are usually located at the terminal end plate motor (the motor end plate). When a nerve impulse arrives at the neuromuscular junction, approximately 125 bags of acetylcholine release from synaptic terminals into the crack. When the action potential spreads throughout the terminal, there will be diffusion of calcium ions into the interior of the terminal. Calcium ions then have the effect of acetylcholine vesicles is expected to attract. Some will be incorporated into the membrane vesicles and released into the nerve asetilkolinnya synaptic gap. Release of acetylcholine diffuses throughout the synapse and bind to the acetylcholine receptors (AChRs) in the post synaptic membrane. With a biochemist at the neuromuscular junction whole process takes place in six stages are considered, namely:
1. Acetyl choline synthesis occurs at the nerve terminal cytosolic enzyme choline acetyltransferase using catalyzed reaction follows: Acetyl-CoA + choline + CoA à Acetylcholine
2. Acetylcholine then inserted into a small vesicle-membrane bound particles called sinap and stored in vesicles.
3. The release of acetylcholine from synaptic vesicles to the gap represents the next stage. This occurs through eksositosis involving vesicle fusion with the membrane presinaptik. In the resting state quanta, single (about 10,000 transmitter molecules that may be appropriate to the content of synaptic vesicles) will be released spontaneously, resulting in a small miniature endplate potential. If the end of the depolarization caused by nerve experienced transmission of nerve impulses, the process will open the channels Ca2 + sensitive to voltage, which allows the entry of Ca2 + from the space into synaptic nerve terminals. This Ca2 + ions play an important role in asitilkolin eksositosis release (the contents of about 125 vesicles) into the cavity of the synapse.
4. Acetylcholine is released will spread rapidly in the synaptic gap to receptor within the folds of the links (junctional folds), are an important part containing the motor end plate acetylcholine receptor (AChR) with high density and very dense with nerve terminal. If the two molecules bound to the acetylcholine receptor, the receptor will change shape by opening the channels of the receptor that allows the flow of cations across the membrane. The entry of Na + ions will cause depolarization of muscle membrane, forming an end plate potential. This situation will then lead to muscle membrane depolarization and action potential occurred near transmitted along nerve fibers causing muscle contraction.
5. If the channel is closed, acetylcholine will rot and hydrolyzed by the enzyme acetylcholinesterase which catalyzes the following reaction: Acetylcholine + H ¬ ¬ à Acetate + 2o Kolin.Enzim important to have large quantities in the cavity of synaptic basal lamina
6. Recycling choline into nerve terminals via an active transport mechanism in which the protein can be reused for the synthesis of acetylcholine.
Each of acetylcholine receptors are large protein complexes with channels that will open soon after the compliance of acetylcholine. This complex consists of five protein subunits, yatiu 2 alpha protein, and one each protein, beta, delta and gamma. Acetylcholine compliance allows the sodium can move easily across the channel, so that will happen partial depolarization of the post-synaptic membranes. This event will cause a change in local potential at the muscle fiber membrane called excitatory postsynaptic potential (the potential end of the plate). When opening the door of sodium is sufficient, there will be action potentials in the muscle membrane which in turn causes muscle contraction.
Some properties of acetylcholine receptors at the neuromuscular junction are as follows:
• Represents nikotinik receptor (nicotine receptor agonists are)
• It is a membrane glycoprotein with a molecular weight of about 275 kDa.
• Contains five subunits, consist of?
• Only a subunit? acetylcholine binds with high affinity.
• Two acetylcholine molecules must bind to open ion channels, which allow the flow of either Na + or K +.
• Can the snake-binding Bungarotoksin? Subunits closely, and can be used to label as a receptor or ligand berafinitas to fix it.
• autoantibody to the receptor, including the cause of miastenia graphics.
Pathophysiology
Immunogenic mechanisms play a very important role in the pathophysiology miastenia gravis. Clinical observations that support this, including autoimmune disorders associated with the incidence of patients who suffer miastenia gravis, such as autoimmune thyroiditis, systemic lupus erythematosus, rheumatoid arthritis, and others.
Starting in 1960, has demonstrated how autoantibodi miastenia gravis patients in the serum directly to constituents in the muscle. This is what plays an important role in weakening the muscles of patients with miatenia gravis. No doubt, that nikotinik acetylcholine receptor antibody on the main causes of muscle weakness in patients with miastenia gravis. Autoantibodi against acetylcholine receptor (anti-AChRs) has been detected in the serum of 90% of patients suffering from acquired gravis gravis general.
Appropriate mechanisms of loss of tolerance to the acetylcholine receptor imunologic miastenia gravis patients are not fully understood. Miastenia gravis can be said as a "disease associated with B cells", in which antibodies are the product of B cells in fact against the acetylcholine receptor. The role of T cells in the pathogenesis miastenia gravis began increasingly prominent. Thymus is the central organ of the immune abnormalities associated with T cell hyperplasia of the thymus as the thymus or thymoma, usually appears earlier in patients with symptoms miastenik. In miastenia gravis patients, IgG antibodies consist of a variety of different subklas, where one antibody directly against the main immunogenic region on the alpha subunit. Alpha subunit is also the acetylcholine binding site. Association of acetylcholine receptor antibodies on acetylcholine receptor would lead to obstruction of neuromuscular transmission in several ways, including: cross-acetylcholine receptor anti-acetylcholine receptor antibodies and reducing the number of acetylcholine receptors at the neuromuscular junction by way of destroying the connection of the bonds at post synaptic membrane, thereby reducing the surface area that can be used for the insertion of newly synthesized acetylcholine receptors.
CLINICAL SYMPTOMS
Miastenia gravis characterized by fluctuating skeletal muscle weakness and this weakness will increase every time they move. Patients will feel very weak muscles in the day and this weakness will be reduced if the rest of the patient. Miastenia gravis clinical symptoms include:
a. Weakness in the muscles or ptosis ekstraokular
Ptosis, which is one symptom of okulomotorius nerve paralysis, the main complaint seing miastenia gravis patients. Although miastenia gravis on unclear palpebra Levator muscle paralysis, but sometimes the eye muscles are still moving normally. But in advanced stages of ocular muscle paralysis on both sides will complete ptosis miastenia gravis. bulbar muscle weakness are also common, followed by weakness in flexion and extension of the head. Patients with muscle weakness gets worse the longer it will. weakness will spread from the ocular muscles, facial muscles, neck muscles, the muscles of extremities. From time to time can also arise from the masseter muscle weakness so difficult for the patient's mouth shut. But they can also arise from the weakness of the muscles of the pharynx, tongue, Lissoclinum pallatum, and larynx so that the resulting difficulty swallowing and speaking. Paresis of Lissoclinum pallatum will cause nasal voice. Also if the patient drink water, water can get out of his nose.
CLASSIFICATION MIASTENIA Gravis
According to the Myasthenia Gravis Foundation of America (MGFA), berikut7 miastenia gravis can be classified as:
a. First class
The existence of the weakness of ocular muscles, weakness at the time of closing the eyes, and other muscles of normal strength.
b. Class II
There are more severe ocular muscle weakness, and mild muscle weakness in muscles other than ocular.
c. Class IIa
Affect axial muscles, limbs, or both. There are also mild weakness of oropharyngeal muscles.
d. Class IIb
Affecting oropharyngeal muscles, respiratory muscles or both. Weakness in leg muscles and axial muscles are lighter than grade IIA.
e. Class III
There are serious weaknesses in the ocular muscles. While other muscles in addition to moderate muscle weakness experienced eye.
f. Class IIIA
Affecting the leg muscles, axial muscles, or both, is very dominant. There was mild weakness of oropharyngeal muscles.
g. Class IIIB
Affect oropharyngeal muscles, respiratory muscles, or both, is very dominant. There is weakness of leg muscles, axial muscles, or both, in light level.
h. Class IV
Other than experience severe muscle weakness in the degree of ocular muscles, whereas the ocular muscle weakness experienced in various degrees.
i. Class IVA
With primarily affects the muscles or limbs and axial muscles. oropharyngeal muscle weakness is experienced in mild degrees.
j. Class IVb
Affecting the oropharyngeal muscles, respiratory muscles or both, the main thing. There is also a weakness in the muscles of limbs, axial muscles, or both with a mild degree. Patients using a feeding tube without intubation performed.
k. Class V
Terintubasi patients, with or without mechanical ventilation.
Usually symptoms closet gravis ptosis and strabismus miastenia will not be visible in the morning. At night or during hot weather, symptoms will appear more clearly. On examination, the muscle appeared somewhat decreased.
Miastenia gravis can also be grouped with a more simple way as below ini3:
a. Miastenia gravis with mild ptosis or diplopia.
b. Miastenia gravis by ptosis, diplopi, and weakness of the muscles for chewing, swallowing and speaking. tubuhpun members can participate Muscles become weak. Breathing is not affected.
c. Gravis Miastenia happens fast with muscle weakness okulobulbar. Breathing is not affected. Patients can die.
DIAGNOSIS MIASTENIA Gravis
a. Diagnosis Enforcement Miastenia Gravis
With a thorough physical examination should be performed to diagnose miastenia gravis. muscle weakness can occur in different degrees, typically in the proximal part of the body and symmetrical on both left and right leg. tendon reflexes are usually still within normal limits.
Miastenia gravis is usually always accompanied by weakness of facial muscles. Bilateral facial muscle weakness will cause the face like a mask with ptosis and horizontal smile.
bulbar muscle weakness are also common in patients with miastenia gravis. On physical examination, there was muscle weakness of the palate, which causes sufferers sounds like being in the nose (nasal twang to the voice) and regurgitation of food, especially the character of liquid into the patient's nose. In addition, miastenia gravis patients will have difficulty in chewing and swallowing food, so it can happen menyebabbkan fluid aspiration when drinking cough and choke. Weakness in the muscles of the jaw causes miastenia gravis patients difficult to close the mouth, chin so that the patient should be kept continuous with his hands. neck muscles are also experiencing weakness, so that an interruption occurs during flexion and extension of the neck.
Limb muscles from certain experiences more often than the weakness of the muscles of the body of another member, whereby the muscles of your upper body more frequently experience muscle weakness compared with the lower limb. Deltoid muscle function and extension at the wrist and fingers often experience weakness. Triceps muscles more commonly affected than the biceps. At the bottom of the foot, weakness often occur when doing hip flexion, and dorsiflexion of the toes as compared with the toes do plantarfleksi.
respiratory muscle weakness can result from acute respiratory failure, which is a state of emergency and quick action is required intubation. Intercostal and diaphragm muscle weakness can cause retention of carbon dioxide will cause hypoventilation. pharyngeal muscle weakness may cause airway collapse, strict controls breathing function in patients with acute phase required miastenia gravis.
Muscle weakness usually happens in ekstraokular asymmetrical. Weakness often affect more than one muscle ekstraokular, and not just limited to the muscles that diinervasi by a cranial nerve. This is a very important sign for diagnosing miastenia gravis. The weakness in the lateral and medial rectus muskulus will cause pseudointernuclear ophthalmoplegia, marked by adduction of one eye on the limited ability of the eyes accompanied nistagmus kidnapping.
To miastenia gravis diagnosis, examination may be conducted as follows:
1. Patients were assigned to count out loud. Finally, you will hear his voice grew weaker and less bright. Patients become anartris and afonis.
2. Patients assigned to his eyes blink constantly. Ptosis will occur from time to time. After the patient became hoarse voice or see any ptosis, the patient was told to rest .. Then came that voice will be back better and ptosis was not seen again.
To confirm the diagnosis miastenia gravis, several tests can be conducted between lain3:
1. Tensilon test (edrophonium chloride)
To test tensilon, 2 tensilon mg injected intravenously, if there is a reaction to it again as many as 8 mg was injected intravenously tensilon. Immediately after injection tensilon It should be noted that the muscle is weak, such as eyelid ptosis shows. If that's true weakness is caused by miastenia gravis, ptosis will soon disappear. In uiji weak eyelid should be considered very carefully, because the effectiveness of very short tensilon.
2. Test Prostigmin (neostigmin)
In this test injected 3 cc or 1.5 mg administered intramuscularly merhylsulfat prostigmin (if necessary, were also given atropine ¼ or ½ mg). If that's true weakness is caused by miastenia gravis symptoms such as ptosis, strabismus or other weaknesses will not soon disappear.
3. Kina test
3 given quinine tablets 200 mg. 3 hours and then given another three tablets (each 200 mg per tablet). If that's true weakness is caused by miastenia gravis, later symptoms such as ptosis, strabismus and other people will gain weight. For this test, should be prepared prostigmin injection wells, in order miastenik symptoms do not gain weight.
vis is an autoimmune disorder characterized by abnormal and progressive weakness of skeletal muscle that is used constantly and is accompanied by fatigue during recess beraktivitas.Bila patients, so there is no muscle power will soon recover. This disease occurs due to disruption or synaptic transmission at the neuromuscular junction.
Epidemiology
Miastenia gravis is a rare disease, and can occur at any age. This disease is usually more often seen at the age of 20-50 years. Women more often than men suffer from this disease. Ratio of women and men who suffer miastenia gravis is 6: 4. In women, this disease appears early in life, which is about 28 years, whereas in men, the disease often occurs at the age of 42 years.
ANATOMY, PHYSIOLOGICAL, and biochemical neuromuscular junction
a. Anatomy of the neuromuscular junction
Before an understanding of miastenia gravis, knowledge of anatomy and normal function of the neuromuscular junction is very important. Every normal nerve fibers branched several times and stimulated three to several hundred skeletal muscle fibers. nerve endings to create a connection called the neuromuscular junction or the neuromuscular junction. Part of motor nerve terminals eventually called the ball wide on the terminal, which lies in between the cracks found along nerve fibers. Presinaptik membrane (membrane of the nerve), post-synaptic membrane (membrane of the muscle), and the synapse is a gap to form part of the neuromuscular junction.
b. Neuromuscular Physiology and Bi
ochemistry
Synapse is the gap between the membrane and presinaptik post synaptic membrane. Ranged from 20-30 nanometers wide and filled by a basal lamina, which is a thin layer of reticular fibers as the foam that can be passed by the extracellular fluid by diffusion. Presinaptik terminals containing acetylcholine-containing vesicles in it (ACH). Acetylcholine is synthesized in the cytoplasm terminal, but quickly absorbed into the small number of synaptic vesicles, which are usually located at the terminal end plate motor (the motor end plate). When a nerve impulse arrives at the neuromuscular junction, approximately 125 bags of acetylcholine release from synaptic terminals into the crack. When the action potential spreads throughout the terminal, there will be diffusion of calcium ions into the interior of the terminal. Calcium ions then have the effect of acetylcholine vesicles is expected to attract. Some will be incorporated into the membrane vesicles and released into the nerve asetilkolinnya synaptic gap. Release of acetylcholine diffuses throughout the synapse and bind to the acetylcholine receptors (AChRs) in the post synaptic membrane. With a biochemist at the neuromuscular junction whole process takes place in six stages are considered, namely:
1. Acetyl choline synthesis occurs at the nerve terminal cytosolic enzyme choline acetyltransferase using catalyzed reaction follows: Acetyl-CoA + choline + CoA à Acetylcholine
2. Acetylcholine then inserted into a small vesicle-membrane bound particles called sinap and stored in vesicles.
3. The release of acetylcholine from synaptic vesicles to the gap represents the next stage. This occurs through eksositosis involving vesicle fusion with the membrane presinaptik. In the resting state quanta, single (about 10,000 transmitter molecules that may be appropriate to the content of synaptic vesicles) will be released spontaneously, resulting in a small miniature endplate potential. If the end of the depolarization caused by nerve experienced transmission of nerve impulses, the process will open the channels Ca2 + sensitive to voltage, which allows the entry of Ca2 + from the space into synaptic nerve terminals. This Ca2 + ions play an important role in asitilkolin eksositosis release (the contents of about 125 vesicles) into the cavity of the synapse.
4. Acetylcholine is released will spread rapidly in the synaptic gap to receptor within the folds of the links (junctional folds), are an important part containing the motor end plate acetylcholine receptor (AChR) with high density and very dense with nerve terminal. If the two molecules bound to the acetylcholine receptor, the receptor will change shape by opening the channels of the receptor that allows the flow of cations across the membrane. The entry of Na + ions will cause depolarization of muscle membrane, forming an end plate potential. This situation will then lead to muscle membrane depolarization and action potential occurred near transmitted along nerve fibers causing muscle contraction.
5. If the channel is closed, acetylcholine will rot and hydrolyzed by the enzyme acetylcholinesterase which catalyzes the following reaction: Acetylcholine + H ¬ ¬ à Acetate + 2o Kolin.Enzim important to have large quantities in the cavity of synaptic basal lamina
6. Recycling choline into nerve terminals via an active transport mechanism in which the protein can be reused for the synthesis of acetylcholine.
Each of acetylcholine receptors are large protein complexes with channels that will open soon after the compliance of acetylcholine. This complex consists of five protein subunits, yatiu 2 alpha protein, and one each protein, beta, delta and gamma. Acetylcholine compliance allows the sodium can move easily across the channel, so that will happen partial depolarization of the post-synaptic membranes. This event will cause a change in local potential at the muscle fiber membrane called excitatory postsynaptic potential (the potential end of the plate). When opening the door of sodium is sufficient, there will be action potentials in the muscle membrane which in turn causes muscle contraction.
Some properties of acetylcholine receptors at the neuromuscular junction are as follows:
• Represents nikotinik receptor (nicotine receptor agonists are)
• It is a membrane glycoprotein with a molecular weight of about 275 kDa.
• Contains five subunits, consist of?
• Only a subunit? acetylcholine binds with high affinity.
• Two acetylcholine molecules must bind to open ion channels, which allow the flow of either Na + or K +.
• Can the snake-binding Bungarotoksin? Subunits closely, and can be used to label as a receptor or ligand berafinitas to fix it.
• autoantibody to the receptor, including the cause of miastenia graphics.
Pathophysiology
Immunogenic mechanisms play a very important role in the pathophysiology miastenia gravis. Clinical observations that support this, including autoimmune disorders associated with the incidence of patients who suffer miastenia gravis, such as autoimmune thyroiditis, systemic lupus erythematosus, rheumatoid arthritis, and others.
Starting in 1960, has demonstrated how autoantibodi miastenia gravis patients in the serum directly to constituents in the muscle. This is what plays an important role in weakening the muscles of patients with miatenia gravis. No doubt, that nikotinik acetylcholine receptor antibody on the main causes of muscle weakness in patients with miastenia gravis. Autoantibodi against acetylcholine receptor (anti-AChRs) has been detected in the serum of 90% of patients suffering from acquired gravis gravis general.
Appropriate mechanisms of loss of tolerance to the acetylcholine receptor imunologic miastenia gravis patients are not fully understood. Miastenia gravis can be said as a "disease associated with B cells", in which antibodies are the product of B cells in fact against the acetylcholine receptor. The role of T cells in the pathogenesis miastenia gravis began increasingly prominent. Thymus is the central organ of the immune abnormalities associated with T cell hyperplasia of the thymus as the thymus or thymoma, usually appears earlier in patients with symptoms miastenik. In miastenia gravis patients, IgG antibodies consist of a variety of different subklas, where one antibody directly against the main immunogenic region on the alpha subunit. Alpha subunit is also the acetylcholine binding site. Association of acetylcholine receptor antibodies on acetylcholine receptor would lead to obstruction of neuromuscular transmission in several ways, including: cross-acetylcholine receptor anti-acetylcholine receptor antibodies and reducing the number of acetylcholine receptors at the neuromuscular junction by way of destroying the connection of the bonds at post synaptic membrane, thereby reducing the surface area that can be used for the insertion of newly synthesized acetylcholine receptors.
CLINICAL SYMPTOMS
Miastenia gravis characterized by fluctuating skeletal muscle weakness and this weakness will increase every time they move. Patients will feel very weak muscles in the day and this weakness will be reduced if the rest of the patient. Miastenia gravis clinical symptoms include:
a. Weakness in the muscles or ptosis ekstraokular
Ptosis, which is one symptom of okulomotorius nerve paralysis, the main complaint seing miastenia gravis patients. Although miastenia gravis on unclear palpebra Levator muscle paralysis, but sometimes the eye muscles are still moving normally. But in advanced stages of ocular muscle paralysis on both sides will complete ptosis miastenia gravis. bulbar muscle weakness are also common, followed by weakness in flexion and extension of the head. Patients with muscle weakness gets worse the longer it will. weakness will spread from the ocular muscles, facial muscles, neck muscles, the muscles of extremities. From time to time can also arise from the masseter muscle weakness so difficult for the patient's mouth shut. But they can also arise from the weakness of the muscles of the pharynx, tongue, Lissoclinum pallatum, and larynx so that the resulting difficulty swallowing and speaking. Paresis of Lissoclinum pallatum will cause nasal voice. Also if the patient drink water, water can get out of his nose.
CLASSIFICATION MIASTENIA Gravis
According to the Myasthenia Gravis Foundation of America (MGFA), berikut7 miastenia gravis can be classified as:
a. First class
The existence of the weakness of ocular muscles, weakness at the time of closing the eyes, and other muscles of normal strength.
b. Class II
There are more severe ocular muscle weakness, and mild muscle weakness in muscles other than ocular.
c. Class IIa
Affect axial muscles, limbs, or both. There are also mild weakness of oropharyngeal muscles.
d. Class IIb
Affecting oropharyngeal muscles, respiratory muscles or both. Weakness in leg muscles and axial muscles are lighter than grade IIA.
e. Class III
There are serious weaknesses in the ocular muscles. While other muscles in addition to moderate muscle weakness experienced eye.
f. Class IIIA
Affecting the leg muscles, axial muscles, or both, is very dominant. There was mild weakness of oropharyngeal muscles.
g. Class IIIB
Affect oropharyngeal muscles, respiratory muscles, or both, is very dominant. There is weakness of leg muscles, axial muscles, or both, in light level.
h. Class IV
Other than experience severe muscle weakness in the degree of ocular muscles, whereas the ocular muscle weakness experienced in various degrees.
i. Class IVA
With primarily affects the muscles or limbs and axial muscles. oropharyngeal muscle weakness is experienced in mild degrees.
j. Class IVb
Affecting the oropharyngeal muscles, respiratory muscles or both, the main thing. There is also a weakness in the muscles of limbs, axial muscles, or both with a mild degree. Patients using a feeding tube without intubation performed.
k. Class V
Terintubasi patients, with or without mechanical ventilation.
Usually symptoms closet gravis ptosis and strabismus miastenia will not be visible in the morning. At night or during hot weather, symptoms will appear more clearly. On examination, the muscle appeared somewhat decreased.
Miastenia gravis can also be grouped with a more simple way as below ini3:
a. Miastenia gravis with mild ptosis or diplopia.
b. Miastenia gravis by ptosis, diplopi, and weakness of the muscles for chewing, swallowing and speaking. tubuhpun members can participate Muscles become weak. Breathing is not affected.
c. Gravis Miastenia happens fast with muscle weakness okulobulbar. Breathing is not affected. Patients can die.
DIAGNOSIS MIASTENIA Gravis
a. Diagnosis Enforcement Miastenia Gravis
With a thorough physical examination should be performed to diagnose miastenia gravis. muscle weakness can occur in different degrees, typically in the proximal part of the body and symmetrical on both left and right leg. tendon reflexes are usually still within normal limits.
Miastenia gravis is usually always accompanied by weakness of facial muscles. Bilateral facial muscle weakness will cause the face like a mask with ptosis and horizontal smile.
bulbar muscle weakness are also common in patients with miastenia gravis. On physical examination, there was muscle weakness of the palate, which causes sufferers sounds like being in the nose (nasal twang to the voice) and regurgitation of food, especially the character of liquid into the patient's nose. In addition, miastenia gravis patients will have difficulty in chewing and swallowing food, so it can happen menyebabbkan fluid aspiration when drinking cough and choke. Weakness in the muscles of the jaw causes miastenia gravis patients difficult to close the mouth, chin so that the patient should be kept continuous with his hands. neck muscles are also experiencing weakness, so that an interruption occurs during flexion and extension of the neck.
Limb muscles from certain experiences more often than the weakness of the muscles of the body of another member, whereby the muscles of your upper body more frequently experience muscle weakness compared with the lower limb. Deltoid muscle function and extension at the wrist and fingers often experience weakness. Triceps muscles more commonly affected than the biceps. At the bottom of the foot, weakness often occur when doing hip flexion, and dorsiflexion of the toes as compared with the toes do plantarfleksi.
respiratory muscle weakness can result from acute respiratory failure, which is a state of emergency and quick action is required intubation. Intercostal and diaphragm muscle weakness can cause retention of carbon dioxide will cause hypoventilation. pharyngeal muscle weakness may cause airway collapse, strict controls breathing function in patients with acute phase required miastenia gravis.
Muscle weakness usually happens in ekstraokular asymmetrical. Weakness often affect more than one muscle ekstraokular, and not just limited to the muscles that diinervasi by a cranial nerve. This is a very important sign for diagnosing miastenia gravis. The weakness in the lateral and medial rectus muskulus will cause pseudointernuclear ophthalmoplegia, marked by adduction of one eye on the limited ability of the eyes accompanied nistagmus kidnapping.
To miastenia gravis diagnosis, examination may be conducted as follows:
1. Patients were assigned to count out loud. Finally, you will hear his voice grew weaker and less bright. Patients become anartris and afonis.
2. Patients assigned to his eyes blink constantly. Ptosis will occur from time to time. After the patient became hoarse voice or see any ptosis, the patient was told to rest .. Then came that voice will be back better and ptosis was not seen again.
To confirm the diagnosis miastenia gravis, several tests can be conducted between lain3:
1. Tensilon test (edrophonium chloride)
To test tensilon, 2 tensilon mg injected intravenously, if there is a reaction to it again as many as 8 mg was injected intravenously tensilon. Immediately after injection tensilon It should be noted that the muscle is weak, such as eyelid ptosis shows. If that's true weakness is caused by miastenia gravis, ptosis will soon disappear. In uiji weak eyelid should be considered very carefully, because the effectiveness of very short tensilon.
2. Test Prostigmin (neostigmin)
In this test injected 3 cc or 1.5 mg administered intramuscularly merhylsulfat prostigmin (if necessary, were also given atropine ¼ or ½ mg). If that's true weakness is caused by miastenia gravis symptoms such as ptosis, strabismus or other weaknesses will not soon disappear.
3. Kina test
3 given quinine tablets 200 mg. 3 hours and then given another three tablets (each 200 mg per tablet). If that's true weakness is caused by miastenia gravis, later symptoms such as ptosis, strabismus and other people will gain weight. For this test, should be prepared prostigmin injection wells, in order miastenik symptoms do not gain weight.





{kind=link}
0 komentar:
Post a Comment